Patient Case:
A 62-year-old female presents to the ED with left lower extremity pain and swelling and is diagnosed with a LLE deep vein thrombosis (DVT) on ultrasound. The patient’s past medical history is significant for hypertension and she takes amlodipine at home. Laboratory values, pulse oximetry, and vital signs are within normal limits. The ED physician approaches you about discharge anticoagulation options and asks for a recommendation. Which agent would you recommend for outpatient management of this patient’s DVT?
Background:
EM pharmacists are frequently involved in the drug selection, ordering, dose verification, and patient education regarding anticoagulants in the ED for admitted and discharge patients. We are in a unique situation in which we work closely with providers everyday to make our recommendation on the the best option for individual patients based on patient-specific factors, cost, potential drug interactions, and balancing safety with efficacy.
Since FDA approval of dabigatran in 2010, the NOAC class of anticoagulants has rapidly gained popularity. Zhu et al.1 recently published data concerning NOAC use among atrial fibrillation (AF) patients between 2010 and 2017. In 2017, they identified more than 7500 new patients started on an oral anticoagulant and 79% received a NOAC compared to 21% with warfarin. Of those NOACs, apixaban was the most common agent at 50.1%, followed by rivaroxaban at 25%, and dabigatran at 3.8%. With so many options available, how do you choose which agent to send your patient home on?
Efficacy and Safety Data
Based on the results of the industry sponsored trials, we know apixaban and rivaroxaban are non-inferior to warfarin,2-5 but what about compared to each other?
Lopez-Lopez et al. completed a systematic review and meta-analysis of all available Phase II and Phase III superiority and non-inferiority trials of NOACs and VKAs for stroke prevention in patients with AF.6 The best part about this study (aside from being open-access) was they actually compared each agent against each other. In terms of efficacy, rivaroxaban 20 mg daily was shown to be no different than apixaban 5 mg twice-daily in terms of stroke and systemic embolism, ischemic stroke, myocardial infarction, or all-cause mortality (see Table 1). When looking at safety outcomes, rivaroxaban was shown to increase the risk for major bleeding, GI hemorrhage, and clinically relevant bleeding compared to apixaban with no difference in intracranial hemorrhage (see Table 2).
Table 1: Indirect efficacy comparison of rivaroxaban and apixaban
|
|
Stroke or systemic embolism
|
Ischemic stroke
|
Myocardial infarction
|
All-cause mortality
|
|
Rivaroxaban 20 mg daily vs apixaban 5 mg BID,
OR (95% CI)
|
1.11
(0.87-1.41)
|
1.01
(0.74-1.38)
|
0.92
(0.63-1.34)
|
0.94
(0.76-1.17)
|
Table 2: Indirect safety comparison of rivaroxaban and apixaban
|
|
Major Bleeding
|
Intracranial hemorrhage
|
Gastrointestinal hemorrhage
|
Clinically relevant bleeding
|
|
Rivaroxaban 20 mg daily vs
apixaban 5 mg BID,
OR (95% CI)
|
1.45
(1.19-1.78)
|
1.55
(0.97-2.49)
|
1.66
(1.19-2.33)
|
1.53
(1.33-1.75)
|
What about real-world data? We know that Phase II and Phase III clinical trial results don’t always translate equally to the general public, so how might these numbers change? Larsen et al. completed a large, retrospective, Danish study which extracted prescription data from three nationwide databases.7 Patients with AF were identified by first time purchases of NOACs or warfarin between 2011 and 2015. More than 122,000 patients were identified, and after exclusions approximately 62,000 patients were analyzed. Patients were mostly males aged 68 to 72 years with a CHADS2-VASC Score of 2.2-2.8. When compared to warfarin, there was no difference in hazard ratios (HR) for ischemic stroke or ischemic stroke + systemic embolism for apixaban compared to warfarin. Rivaroxaban showed a reduced HR compared to warfarin with the composite endpoint of ischemic stroke + systemic embolism (with the 95% CI upper limit at 0.99); but no difference in ischemic stroke alone. The composite endpoint of ischemic stroke + systemic embolism + death favored apixaban and rivaroxaban compared to warfarin (see Table 3).
In terms of safety outcomes including death, any bleeding event, and major bleeding events, HRs were lower with apixaban compared to warfarin, but not with rivaroxaban compared to warfarin (see Table 3). These trends favoring apixaban also continued when patients were stratified based on age of <65 or >65 years. Interestingly, intracranial hemorrhages with apixaban were no different compared to warfarin, but actually lower with rivaroxaban compared to warfarin in this cohort (see Table 3).
However, the original AMPLIFY2 and ARISTOLE4 trials both showed lower intracranial hemorrhage risk with apixaban compared to warfarin. Additionally, this systematic review and meta-analysis showed a lower ICH risk with apixaban vs warfarin and no difference between rivaroxaban vs warfarin.8 Taken together, I give the slight advantage to the RCT data over the Danish registry data given multiple trials with the same results and trust that apixaban is safer than warfarin.
Table 3: Real-world comparison of NOACs to warfarin
|
Apixaban vs Warfarin
HR (95% CI)<
/div> |
Rivaroxaban vs Warfarin
HR (95% CI)
|
|
Ischemic stroke + systemic embolism
|
1.08 (0.91-1.27)
|
0.83 (0.69-0.99)
|
|
Ischemic stroke
|
1.11 (0.904-1.3)
|
0.86 (0.72-1.04)
|
|
Ischemic stroke +
systemic embolism + death
|
0.79 (0.7-0.88)
|
0.87 (0.79-0.96)
|
|
Death
|
0.62 (0.56-0.75)
|
0.9 (0.82-1.03)
|
|
Any bleeding event
|
0.63 (0.53-0.76)
|
0.99 (0.86-1.14)
|
|
Major bleeding
|
0.61 (0.49-0.75)
|
1.06 (0.91-1.23)
|
|
Intracranial hemorrhage
|
0.72 (0.42-1.24)
|
0.56 (0.34-0.9)
|
Granted these data do not represent a direct, head-to head comparison between apixaban and ri
varoxaban (and neither did the previous study as that data was generated via an indirect method). However, when the real world data closely mirrors clinical trial data with such large study populations, I feel fairly confident generalizing these overall trends when comparing apixaban and rivaroxaban against each other in terms of efficacy and safety.
Renal dosing concerns:
Both apixaban and rivaroxaban require renal dose adjustments. It is very important to note the dose cutoffs for each agent vary depending on the indication (AF vs VTE). Rivaroxaban can be utilized for AF patients with a CrCl > 15 ml/min but for VTE patients the cutoff is increased to a CrCl > 30 ml/min. Apixaban’s adjustments are based on serum creatinine and not necessarily a specific CrCl cutoff. Additionally, there is some data with reduced-dose apixaban showing similar AUCs in patients on hemodialysis as standard doses in patients with normal renal function.9 As only 4% of the drug was removed during a 4-hour HD session, it is unclear if the same dosing scheme of 2.5 mg BID could be applied to non-dialysis patients with significant chronic renal impairment.
Overall, check your drug references to ensure proper dosing given the varying cutoffs in CrCl, Scr, age, and indication used. If you have a patient in your ED with renal disease and for some reason they cannot (or refuse to) be treated with warfarin, choosing an alternative oral agent may be difficult. Among AF patients, rivaroxban’s lower CrCl cutoff of 15 ml/min should encompass a large number of potential patients. Alternatively, given the PK data of apixaban in HD patients, you could consider having a conversation with the provider and patient to decide if apixaban would be worth a try.
Drug interaction considerations:
Compared to warfarin, both apixaban and rivaroxaban have less concerns for drug-drug interactions. However, significant interactions do remain and the ED pharmacist should be vigilant to identify and correct such interactions. Both agents are substrates of CYP3A4 and P-glycoprotein (see Table 4 and Table 5). The most concerning interaction for either agent is with diltiazem and apixaban as is not uncommon for patients with atrial fibrillation to be maintained on diltiazem for rate control and therefore need long term anticoagulation. It’s unknown if the approximate 40% increase in apixaban AUC has any clinical significance, but for elderly patients, or those with a high bleeding risk, this combination should likely be avoided.
Table 4: Drug interactions with apixaban10,11
|
Drug
|
Dose
|
Change in apixaban AUC
|
|
Diltiazem
|
360 mg x10 days
|
↑ 40%
|
|
Ketoconazole
|
400 mg x6 days
|
↑ 100%
|
|
Naproxen
|
500 mg, single dose
|
↑ 50%
|
|
Rifampin
|
600 mg x11 days
|
↓ 54%
|
Table 5: Drug interactions with rivaroxaban12
|
Drug
|
Dose
|
Change in rivaroxaban AUC
|
|
Clarithromycin
|
500 mg BID x5 days
|
↑ 54%
|
|
Erythromycin
|
500 mg TID x5 days
|
↑ 34%
|
|
Ketoconazole
|
200 mg x3 days
|
↑ 53%
|
|
Ketoconazole
|
400 mg x5 days
|
↑ 2.6-fold
|
|
Rifampin
|
150 mg, 300 mg, 450 mg, then 600 mg x4 days
|
↓ 49%
|
|
Ritonavir
|
600 mg BID x6 days
|
↑ 2.5-fold
|
Cost considerations:
Given the relative “newness” of the NOACs, generic equivalents are not yet available. Therefore, as can be expected, these medications can be expensive. However, as they are no longer brand new, a larger percentage of private insurance and some state’s Medicaid Formularies will cover at least one NOAC. Additionally, cost-effectiveness analyses have shown favorable results with NOACs compared to warfarin, with apixaban conferring the greatest cost savings.13,14
In my home state of Colorado, the Medicaid Preferred Drug List still has warfarin as its first line option. However, rivaroxaban is a “preferred” agent, albeit second-line. Patients must meet some eligibility criteria to receive coverage, but we have not encountered any problems so far when properly selecting patients for discharge on rivaroxaban.
Most private insurance companies will cover at least one NOAC, likely more. According to Eliquis’s website, almost 95% of patients nationwide “have access to Eliquis.” They even have a tool for people to enter their state or ZIP code to find common prescription insurance plans in those areas to see if coverage is an option.
Luckily, our outpatient pharmacies associated with the hospitals have the ability to offer the first 30-days of therapy for either apixaban or rivaroxaban at no cost to the patient through manufacturer-sponsored programs. Although this is classic “drug dealing behavior,” we take advantage as frequently as possible. This one month of free therapy likely increases compliance which in turn would hopefully decrease the risk for return visits related to thromboembolic events. Additionally, the free month allows the patient to work with their insurance company to verify long term prescription coverage. If a different agent is required, it allows the patient time to meet with their PCP and set up the plan for change. Overall, these free “starter packs” are a great resource. Patients love being able to leave the ED with a 30-day supply of free medication and I’ll take any opportunity for the drug companies to give out free medication. It is unclear if this is available everywhere, but it may not hurt to contact a drug rep in your area to inquire about it if it is not something already available.
Which Agent to Choose?
Several points must be considered when choosing between rivaroxaban and apixaban. Both agents appear to be equally efficacious, but from a safety standpoint, apixaban is the winner in my book. Renal disease may preclude NOAC use, but for some patients rivaroxaban has a lower CrCl cutoff when used for AF than apixaban, so potentially slight advantage there. Cost considerations are very patient- and location-specific. Not mentioned thus far, but worth considering is the BID dosing of apixaban vs daily dosing with rivaroxaban. If patient compliance is a major concern, rivaroxaban will likely be preferred.
|
Consideration
|
Winning Medication
|
|
Efficacy
|
Apixaban = Rivaroxaban
|
|
Safety
|
Apixaban
|
|
Renal Dosing
|
Maybe rivaroxaban, varies by indication
|
|
Drug Interactions
|
Patient specific, unless on diltiazem then maybe favor rivaroxaban
|
|
Cost
|
Variable
|
|
Compliance
|
Rivaroxaban
|
Taken all together, there is a preferred agent in my book. Given similar efficacy, interaction potential, and medication costs, the major deciding factor is safety. Given the fact we don’t have a reliable reversal agent for Xa inhibitors at this point, and knowing the morbidity and mortality associated with major bleeding events, minimizing bleeding risk is of the utmost importance. Apixaban is a clear winner in this regard and is the reason I routinely recommend apixaban over rivaroxaban when both agents are options. In my experience so far, after having a discussion with the patient regarding the improved safety profile weighed against taking the medication twice daily, the vast majority of patients want the safer medication (and I would too). Even if the patient is only on once daily medications at home, you shouldn’t rule out apixaban as they may want the safer option and just because a patient isn’t on a BID therapy doesn’t mean they can’t start now. Have a conversation, discuss the pros and cons, and give your patient all of the information to allow them to make the best decision.
Apixaban is likely the safest oral anticoagulant available, it is equally effective as other NOACs, and with more and more patients eligible for prescription coverage, it is my preferred oral anticoagulant.
Scott Dietrich, PharmD, BCCCP
Emergency Medicine Pharmacist
University of Colorado Health – North Region
*** Dabigatran Disclaimer ***
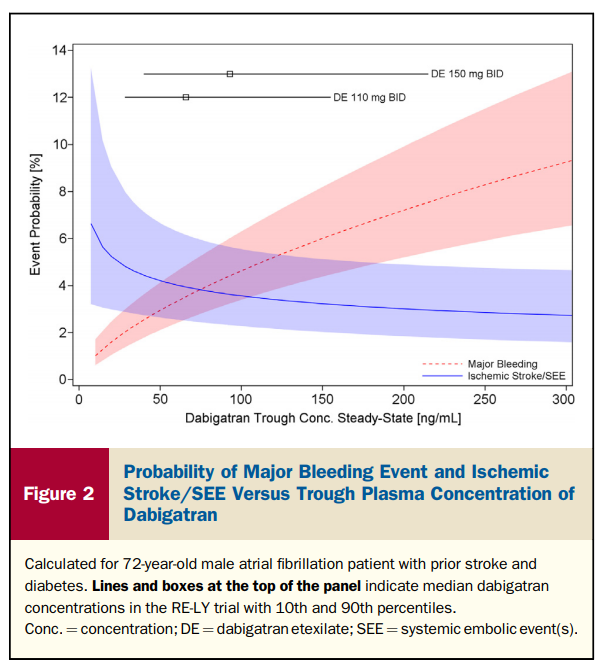
This post only mentions two oral anticoagulants. There are several more Xa inhibitors now available, but they are cost-prohibitive at this point. The other alternative NOAC is dabigatran. As mentioned above, in 2017, < 4% of new NOAC prescriptions were for dabigatran.1 Why? According to a series of 2014 BMJ articles,15,16 the manufacturer of dabigatran, Boehringer Ingelheim, withheld information regarding the potential utility of serum drug monitoring. The confidential internal documents were only made available during the litigation process in the US. Though not published within the initial RE-LY trial, there was a large sub-study within RE-LY that measured serum drug levels.17 While only analyzing patients receiving the 150 mg BID dose of dabigatran, researchers found a extraordinarily wide variability in measured plasma concentrations. After 30 days of therapy, plasma levels ranged from 2.3 ng/ml to a max of 1000 ng/ml. After some adjustments, the researchers determined there was a 5.5-fold variability amongst the population. While there was a negligible decrease in event rates with higher plasma levels, there was a clear linear relationship with increasing bleeding event rates (see figure below).14 Despite this, the drug company did not recommend routine drug level monitoring to ensure safety even though the company determined that measuring and appropriately dosing dabigatran could reduce major bleeding by 30-40%.16 Overall, this medication is not as safe as apixaban6 and given the unethical behavior of the manufacturer and likely requirement for drug level monitoring to ensure safety, I am not recommending dabigatran in anyone at this time.
References:
- Zhu J, Alexander GC, Nazarian S, Segal JB, Wu AW. Trends and variations in oral anticoagulant choice in patients with atrial fibrillation, 2010-2017. Pharmacotherapy. 2018, June [epub ahead of print]
- Agnelli G, Buller HR, Cohen et al. Oral apixaban for the treatment of acute venous thromboembolism (AMPLIFY). NEJM. 2013;29;369(9):789-808
- Prins MH, Lensing AW, Brighton TA, et al. Oral rivaroxaban versus enoxaparin with vitamin K antagonist for the treatment of symptomatic venous thromboembolism in patients with cancer (EINSTEIN-DVT and EINSTEIN-PE): a pooled subgroup analysis of two randomised controlled trials. Lancet Haematology. 2014;1(1):e37-46
- Avezum A, Lopes RD, Schulte PJ, et al. Apixaban in Comparison With Warfarin in Patients With Atrial Fibrillation and Valvular Heart Disease: Findings From the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) Trial. Circulation. 2015;132(8):624-632
- Bansilal S, Bloomgarden Z, Halperin JL, et al. Efficacy and safety of rivaroxaban in patients with diabetes and nonvalvular atrial fibrillation: the Rivaroxaban Once-daily, Oral, Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF Trial). American Heart Journal. 2015;170(4):675-682
- Lopez-Lopez JA, Sterne JA, Thom HHZ, et al. Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis. BMJ. 2017;359:j5058
- Larsen TB, Skoth F, Nielsen PB, Kjaeldgaard JN, Lip GYH. Comparative effectiveness and safety of no
n-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation:propensity weighted nationwide cohort study. BMJ. 2016;353:i3189
- Almutairi AR, Zhou L, Gellad WF, Lee JK, Slack MK, Martin JR, Lo-Ciganic WH. Effectiveness and Safety of Non-vitamin K Antagonist Oral Anticoagulants for Atrial Fibrillationand Venous Thromboembolism: A Systematic Review and Meta-analyses. Clinical Therapeutics. 2017;39(7):1456-1478
- Mavrakanas TA, Samer CF, Nessim SJ, Frisch G, Lipman ML. Apixaban pharmacokinetics at steady state in hemodialysis patients. J Am Soc Nephrology. 2017;28(7):2241-2248
- Horn JR, Hansten PD. Apixaban: an oral anticoagulant. Pharmacy Times. 2013, October. https://www.pharmacytimes.com/publications/issue/2013/october2013/apixaban-an-oral-anticoagulant
- Frost CE, Byon W, Song Y, et al. Effect of ketoconazole and diltiazem on the pharmacokinetics of apixaban, an oral direct factor Xa inhibitor. Br J Clin Pharmacol. 2015;79(5):838-846
- Horn JR, Hansten PD. Rivaroxaban: a new oral anticoagulant. Pharmacy Times. 2012, February. https://www.pharmacytimes.com/publications/issue/2012/february2012/rivaroxaban-a-new-oral-anticoagulant
- Amin A, Stokes M, Makenbaeva D, Wiederkehr D, Wu N, Lawrence JH. Estimated medical cost reductions associated with use of novel oral anticoagulants vs warfarin in a real-world non-valvular atrial fibrillation patient population. J Med Econ. 2014;17(11):771-781
- Amin A, Bruno A, Trocio J, LIn J, Lingohr-Smith M. Comparison of differences in medical costs when new oral anticoagulants are used for the treatment of patients with non-valvular atrial fibrillation and venous thromboembolism vs warfarin or placebo in the US. J Med Econ. 2015;18(6):399-409
- Moore TJ, Cohen MR, Mattison DR. Dabigatran, bleeding, and the regulators. BMJ. 2014;349:g4517
- Cohen D. Dabigatran: how the company withheld important analyses. BMJ. 2014;349:g4670
- Reilly PA, Lehr T, Haertter S, et al. The effect of dabigatran plasma concentrations and patient characteristics on the frequency of ischemic stroke and major bleeding in atrial fibrillation patients: the RE-LY Trial (Randomized Evaluation of Long-Term Anticoagulation Therapy). J Am Coll Cardiol. 2014;63(4):321-328
Share This Story, Choose Your Platform!
Leave A Comment